Anesthesia technology precisely controls unconsciousness in animal tests
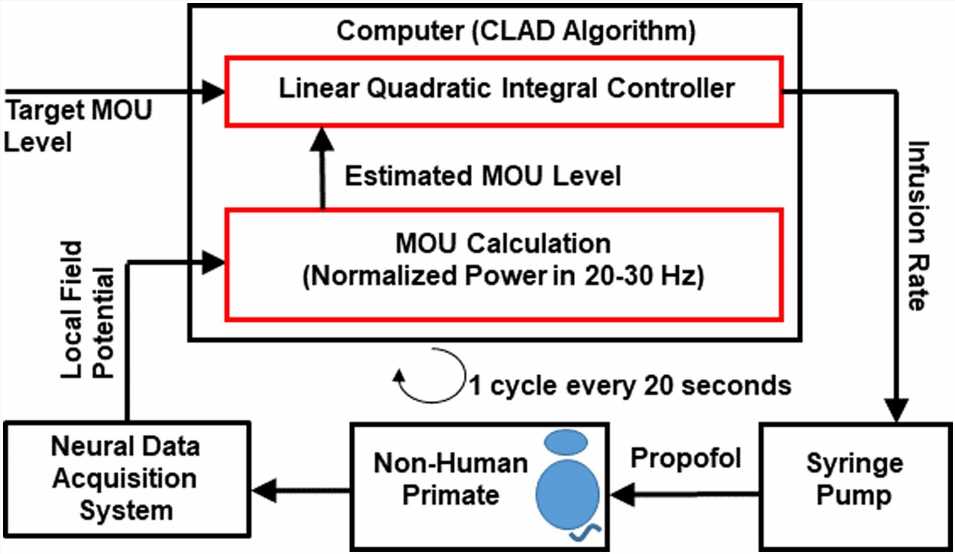
. The controller compares the difference between the target and estimated MOU. Based on that difference the controller changes the infusion rate of the syringe delivering propofol to the NHP. The neural data acquisition system records the LFP, computes an update of the MOU, which is the normalized power in the 20–30 Hz band and the control cycle begins again. The system duty cycle is 20 s. Credit: PNAS Nexus (2023). DOI: 10.1093/pnasnexus/pgad293")
If anesthesiologists had a rigorous means to manage dosing, they could deliver less medicine, maintaining exactly the right depth of unconsciousness while reducing postoperative cognitive side effects in vulnerable groups like the elderly. But with myriad responsibilities for keeping anesthetized patients alive and stable, as well as maintaining their profoundly unconscious state, anesthesiologists don’t have the time without the technology.
To solve the problem, researchers at The Picower Institute for Learning and Memory at MIT and Massachusetts General Hospital have invented a closed-loop system based on brain state monitoring that accurately controls unconsciousness by automating doses of the anesthetic drug propofol every 20 seconds.
The scientists detail the new system and its performance in animal testing in a new study in the journal PNAS Nexus.
“One of the ways to improve anesthesia care is to give just the right amount of drug that’s needed,” said corresponding author Emery N. Brown, Edward Hood Taplin Professor of Medical Engineering and Computational Neuroscience at MIT and an anesthesiologist at MGH. “This opens up the opportunity to do that in a really controlled way.”
In the operating room, Brown monitors the brain state of his patients using electroencephalograms (EEGs). He frequently adjusts dosing based on that feedback, which can cut the amount of drug he uses by as much as half compared to if he just picks a constant infusion rate and sticks with that. Nevertheless, the practice of maintaining dose rather than consciousness level is common because most anesthesiologists are not trained to track brain states and often don’t take time in the operating room to precisely manage dosing.
The new system is not the first closed-loop anesthesia delivery (CLAD) system, Brown said, but it advances the young field in critical ways. Some prior systems merely automate a single, stable infusion rate based on general patient characteristics like height, weight and age but gather no feedback about the actual effect on unconsciousness, said Brown, who is also a member of the Institute for Medical Engineering and Science at MIT and the Warren Zapol Professor in Harvard Medical School.
Others use a proprietary control system that maintains “black box” markers of unconsciousness to vary within a wide range.
The new CLAD system, developed by Brown and his team at the MIT and MGH Brain Arousal State Control Innovation Center (BASCIC), enables very precise management of unconsciousness by making a customized estimate of how doses will affect the subject and by measuring unconsciousness based on brain state. The system uses those measures as feedback to constantly adjust the drug dose.
In the paper, the team demonstrates that the system enabled more than 18 hours of fine-grained consciousness control over the course of nine anesthesia sessions with two animal subjects. Brown Lab research affiliate Sourish Chakravarty and Jacob Donoghue, a former graduate student from the lab of co-senior author and Picower Professor Earl K. Miller, are the paper’s co-lead authors.
Though there is more work to do, the authors write, “We are highly optimistic that the CLAD framework we have established…can be successfully extended to humans.”
How it works
A foundation of the CLAD technology is that it employs a physiologically principled readout of unconsciousness from the brain (in the OR, anesthesiologists typically rely on indirect markers such as heart rate, blood pressure and immobility). The researchers established their brain-based marker by measuring changes in neural spiking activity amid unconsciousness in the animals and the larger scale rhythms that spiking produces, called local field potentials (LFPs).
By closely associating LFP power with spiking-based measures of unconsciousness in the animal subjects, they were able to determine that the total power of LFPs between 20 and 30 Hz is a reliable marker.
The researchers also built into the system a physiologically principled model of the pharmacokinetics (PK) and pharmacodynamics (PD) of propofol, which determines how much drug is needed to alter consciousness and how fast a given dose will have that effect. In the study they show that by coupling the model with the unconsciousness marker they could quickly tune the model for each subject.
“With a few basic recordings of the LFPs as drug is administered you can quickly learn how the subject is responding to the drug,” Brown said.
To manage propofol dosing, every 20 seconds a “linear quadratic integral” controller determines the difference between the measured 20-30 Hz LFP power and the desired brain state (set by the anesthesiologist) and uses the PK/PD model to adjust the infusion of medicine to close the gap.
Initially the team ran computer simulations of how their CLAD system would work under realistic parameters, but then they performed nine, 125-minute-long experiments with two animal subjects. They manually put the animals under and then let the CLAD system take over after about 30 minutes.
In each case the CLAD had to bring the animals to a precise state of unconsciousness for 45 minutes, change to a different level for another 40 minutes, and then bring them back to the original level for 40 more minutes. In every session the system kept the marker very close to the goal levels throughout the duration of the testing.
In other words, rather than a system that automatically maintains the drug dose, the new system automatically maintains the desired level of unconsciousness by updating that dose every 20 seconds.
“The common practice of using constant infusion rates can lead to overdosing,” the researchers wrote. “This observation is particularly relevant for elderly patients who at standard propofol infusion rates readily drift into burst suppression, a profound level of unconsciousness associated with post-operative cognitive disorders.”
In the study the team acknowledges that they have more work to do to advance the technology for human use.
One needed step is basing the system on EEGs, which can be measured via the scalp. Along with that the team will need to determine a marker of unconsciousness based on EEG measurements of human brain rhythms, rather than animal LFPs. Finally, the team wants to extend the system’s capabilities so that it not only maintains unconsciousness, but also helps induce it and helps bring patients back to wakefulness.
More information:
Sourish Chakravarty et al, Closed-loop control of anesthetic state in nonhuman primates, PNAS Nexus (2023). DOI: 10.1093/pnasnexus/pgad293. academic.oup.com/pnasnexus/art … 2/10/pgad293/7330949
Journal information:
PNAS Nexus
Source: Read Full Article


